
By JACOB REIDER
I haven’t blogged about this yet, which surprises me a little since I describe it often.
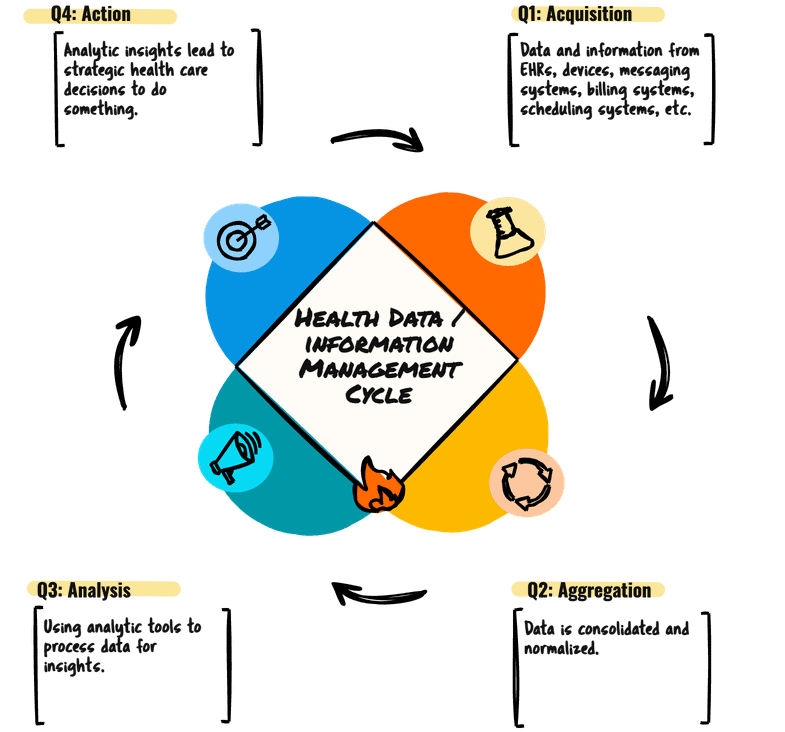
Let’s start with an overview. We can analyze health information through the lens of a life cycle.

The promise of health information technology has been to help us, ideally, achieve optimal health in the people we serve.
The concept at the beginning of the HITECH law was: “ADOPT, CONNECT, IMPROVE.”
These were the three pillars of the Meaningful Use Incentive programs.
Adopt technology so we can connect systems and therefore improve health.
Simple, yes?
Years later, it can be argued that adoption and even connection have been fulfilled (mostly).
But the bridge between measurement and health improvement It is not one that we can easily cross with the current tools available to us.
Because?
Many of the technical solutions, particularly those that promote boardsThey are missing the most crucial piece of the puzzle. They get us close, but then they drop the ball.
And that’s where this “simple” AAAA” model becomes useful.
For data and information to be truly valuable in healthcare, it needs to complete a full cycle.
It is not enough to collect and display. There are four essential steps:
1. Acquire. This is where we collect the raw data and information. EHR inputs, device readings, patient-reported outcomes… the whole range of information flowing into our systems. Please note that I differentiate between dates (transduced representations of the physical world: blood pressure, CBC, the DICOM representation of an MRI, medications actually taken) and information (diagnoses, ideas, symptoms, list of problems, prescribed medications) because the data is reliably true and the information is probably true and possibly inaccurate. We need to properly weigh these two types of inputs, as data is a much better input than information. (I’ll resist the temptation to talk about data being a preferable input to AI models as well… maybe that’s another post).
2. Add. Once acquired, this data and information must be gathered, normalized and cleaned. It’s about making disparate data sources speak the same language, creating a unified repository so we can ask questions about one set of data instead of dozens or hundreds.
3. Analysis. Now we can start to make sense of it. This is where clinical decision support (CDS) begins to take shape – how we can identify trends, flag anomalies, predict risks and highlight opportunities for intervention. The analysis phase is where most current solutions end. A dashboard, an alert, a report… they all dump advice (like a plate of spaghetti) into a human’s lap for them to sort it all out and decide what to do.
Sure… you can see patterns, understand populations and identify areas for improvement… All good things. The maturity of healthcare information technology means that aggregation, normalization and sophisticated analysis are now much more accessible and robust than ever. We no longer need a dozen specialized point solutions to handle each step; Modern platforms can integrate everything. This is good – but not good enough
An analytical dashboard or report, no matter how elegant, is ultimately passive. It shows you the truth, but it’s not like that. do nothing about it.
Act. This is where the rubber hits the road. It is about translating knowledge into tangible interventions. What should happen (or not happen) next?
What good is knowing that a patient is at high risk for readmission if that knowledge does not trigger a specific follow-up protocol, a social work consultation, or an adjusted discharge plan? What is the point of identifying a prescribing pattern if the system does not facilitate a change in practice, provide immediate feedback to physicians, or adjust order sets?
We have relied on human intervention to close this gap. A doctor could see a trend in a report and then initiate a change manually. We see the need to screen and place an order… (one by one).
How sad.
The true power of healthcare IT, especially with the advances we have seen, lies in closing this cycle. We should build systems that not only acquire, aggregate and analyze data, but also facilitate the next best actionprioritizing what is best for the person we serve and (of course) WHO Should you be the recipient of this guide?
Imagine a system that not only flags a potential problem but also:
* Automatically generates a personalized educational document for the patient.
* Suggest an updated medication order (or set of orders) with a single click.
* Schedule follow-up appointments with the corresponding specialists.
* Send a notification to a care coordinator to intervene.
It is not about eliminating human judgment; It’s about enhancing it. It’s about making the right thing the easiest thing to do.
The beauty of this cycle is its iterative nature.
The actions we take then generate new data and information, which feeds back into the “Acquisition” phase, allowing us to continually refine our understanding and improve our interventions. And the faster and more frequently we can go through these four steps, the more responsive, efficient, and patient-centered our healthcare teams will become.
The next time you evaluate a new health IT solution, ask the crucial question: how does this system help us? Act?
Jacob Reider MD is a family physician who previously served as Deputy National Coordinator at ASTP/ONC, CMIO at Allscripts and Albany Medical Center, CEO of Alliance for Better Health, and currently does angel investing, consulting, and pickleballing. Find your occasional thoughts at http://www.docnotes.net which is one of the few blogs older than THCB!

